The Nigerian Urban Reproductive Health Initiative, Phase 2 (NURHI 2), a five-year, Bill & Melinda Gates Foundation-funded project that aims to increase contraceptive use in three Nigerian states, has been busy tackling the issue of health provider bias around family planning. Using the principles of human-centered design (HCD), local NURHI and CCP staff are considering the design challenge: “How might we encourage providers to counsel and offer all clients the full range of contraceptive methods, regardless of the client’s age, marital status, parity, partner consent, or socioeconomic status?”
NURHI has evidence that providers’ own values and beliefs often influence which methods they will or will not offer certain clients. Some, for example, will not offer family planning to young, unmarried women, or hormonal methods to women who have not had children. These biases, whether explicit or implicit, limit contraceptive choice – and in some cases, deny access to contraception completely.
To address this longstanding challenge, NURHI 2 decided to try an HCD approach to learn directly from the people we’re designing for, and co-create a solution that meets their deepest needs – whether they’re aware of those needs or not.
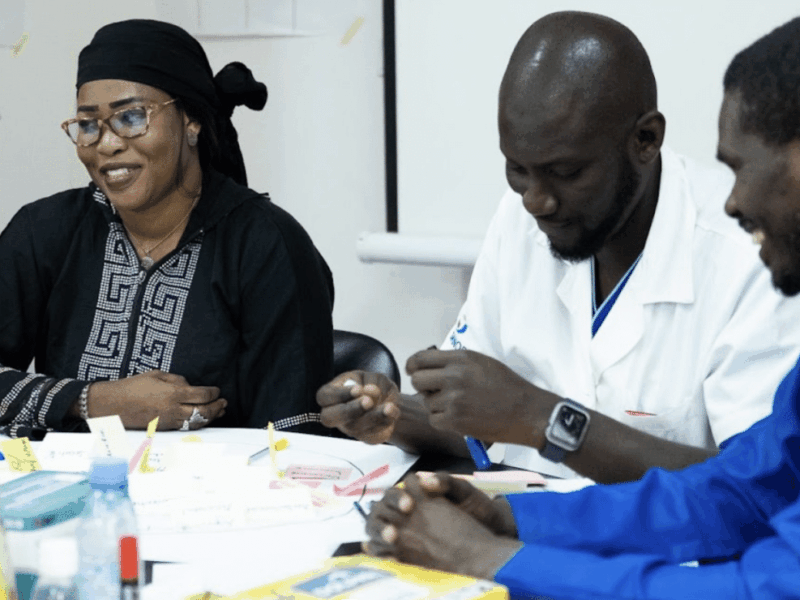
This past November, we conducted an accelerated 4-day design workshop in Lagos that took participants through the entire HCD process, from Inspiration to Ideation and Implementation, using resources adapted primarily from IDEO.org and Design Kit. We brought together a diverse group of participants to help give a range of perspectives and cross-pollinate ideas. Designers included social and behavior change communication (SBCC) professionals, family planning service providers, monitoring and evaluation experts, program managers, State Ministry of Health representatives, advertising agency creatives and radio producers.
Below are our top three moments from the workshop:
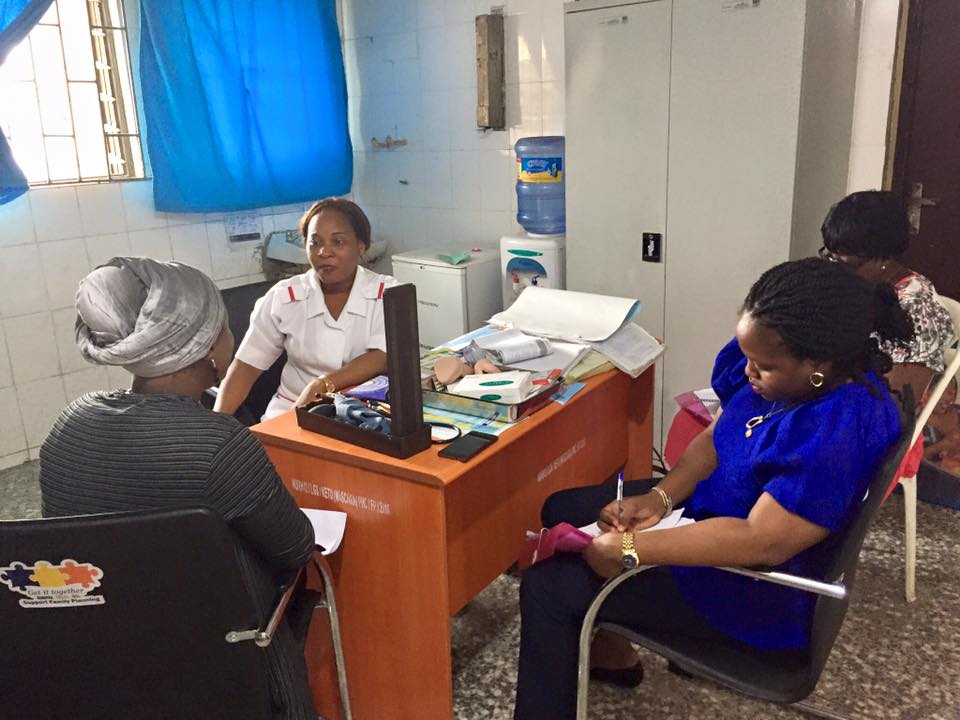
- Inspiration through immersion. After a “crash course” in the mindsets and methods of HCD and a look at the existing evidence around provider bias, we identified the three target audiences we wanted to understand first: family planning service providers, clients and influencers. The team got to work developing interview guides and research tools that would help us dig deeper into why providers are reluctant to give some methods to certain demographics. Groups spent the second day at three different health facilities (two public and one private) interacting with each audience. We used printed images representative of different client categories to spark discussion around how providers would counsel these clients (e.g. an adolescent girl in her school uniform, a young unmarried couple, a recently married couple, a couple with one child, a couple with six children).
 Beyond the conversation starters, teams also asked providers to show them their counseling tools and demonstrate how they use them, received tours of the health facilities and counseling rooms and made observations about the environment. One group was even able to observe a full counseling session, which resulted in a contraceptive implant insertion.
Beyond the conversation starters, teams also asked providers to show them their counseling tools and demonstrate how they use them, received tours of the health facilities and counseling rooms and made observations about the environment. One group was even able to observe a full counseling session, which resulted in a contraceptive implant insertion.- Story sharing and synthesis. We all regrouped in our creative space on the third day, and teams shared their stories from the field. We covered the walls with sticky notes containing observations, quotations and “ah-ha!” moments, then selected the gems among them, categorized these into themes and turned those themes into insight statements. One of our major insights was that while providers receive extensive training and clinical counseling tools that they use frequently and rely on heavily, personal value systems and religious and cultural beliefs still “overrule” medical eligibility criteria in certain cases.
- Ideation and prototyping. Next, it was time to brainstorm. Based on our insights, we formulated the question, “How might we use unconventional methods to shift providers’ perspectives and attitudes?” The ideas started flying. We came up with everything from small twists on the ordinary to the wacky and wild. These included:
- the facilitation of experiences that bring together providers, clients and the community to discuss religious and cultural beliefs around contraception;
- the creation of interactive fora for experiential learning among providers;
- “reward systems” for unbiased providers;
- a “relaxation room” at health facilities where providers could meet informally and exchange ideas;
- an improved values clarification exercise during provider training that more openly addresses the real sources of bias; and,
- the creation of Whatsapp groups that enable continued discussion.
 Beyond the conversation starters, teams also asked providers to show them their counseling tools and demonstrate how they use them, received tours of the health facilities and counseling rooms and made observations about the environment. One group was even able to observe a full counseling session, which resulted in a contraceptive implant insertion.
Beyond the conversation starters, teams also asked providers to show them their counseling tools and demonstrate how they use them, received tours of the health facilities and counseling rooms and made observations about the environment. One group was even able to observe a full counseling session, which resulted in a contraceptive implant insertion. One of our major insights was that while providers receive extensive training and clinical counseling tools that they use frequently and rely on heavily, personal value systems and religious and cultural beliefs still “overrule” medical eligibility criteria in certain cases.
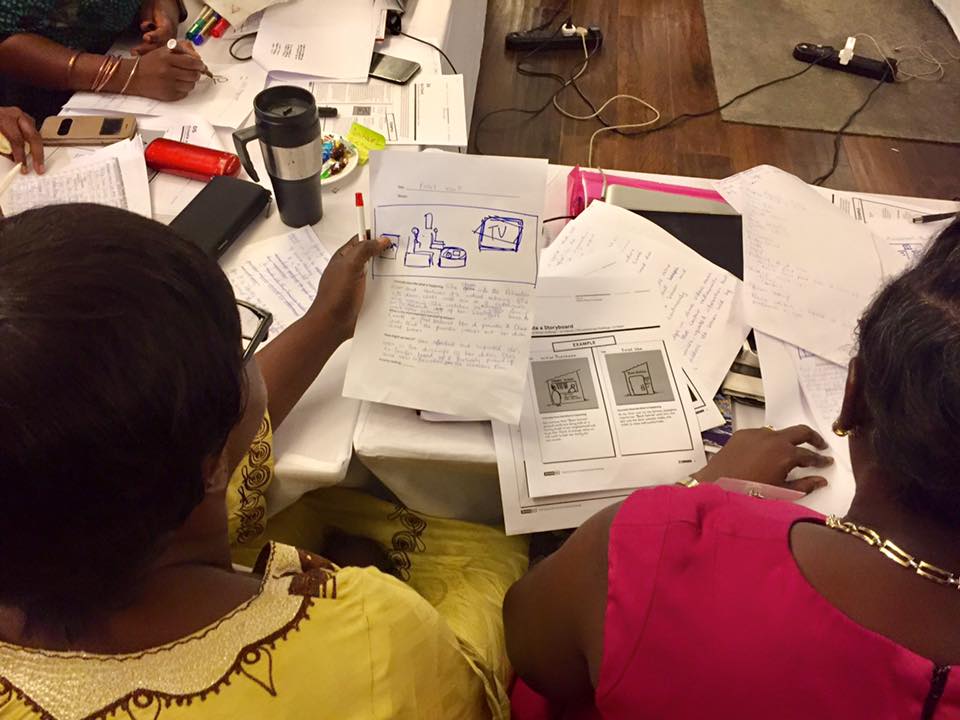
One of our major insights was that while providers receive extensive training and clinical counseling tools that they use frequently and rely on heavily, personal value systems and religious and cultural beliefs still “overrule” medical eligibility criteria in certain cases.Groups then selected their favorite ideas to prototype. We built out the selected ideas first through storyboards, then through mock-ups, and did our first test by sharing the prototypes with each other for feedback.
After the initial HCD workshop in Lagos, newly trained HCD facilitators conducted step-down workshops in Kaduna and Oyo States, where more immersion took place, more sticky notes plastered the walls and more ideas made their way into prototypes. NURHI 2 is currently refining its prototypes for further testing, iteration, and eventual implementation.
This post was written by Jen Orkis, Regional Technical Advisor for Social and Behavior Change Communication. Jen is currently based in Dar es Salaam, Tanzania, supporting CCP projects around the world.